Real-time voice biomarker screening that keeps personnel operation-ready while building psychological resilience at scale.
Manodayam tracks voice biomarkers revealing multi-dimensional mental states beyond traditional scales.
State-of-Mind Dimension |
Voice Biomarkers |
Individual Tracking |
Organizational Trends |
|---|---|---|---|
Emotional Load
|
Vocal energy, pitch variability, speech rate
|
Daily stress trajectories
|
Campus/unit crisis peaks
|
Cognitive Fatigue
|
Learning capacity decline
|
Operational readiness drops
| |
Social Withdrawal
|
Volume modulation, prosody patterns
|
Isolation risk scoring
|
Team cohesion breakdown
|
Neurodegenerative Risk
|
Tremor frequency, vowel formants
|
Early-onset detection
|
Force-wide prevalence
|
Resilience Capacity
|
Recovery speed post-stress, baseline stability
|
Personal growth tracking
|
Institutional wellness ROI
|
12+ months of continuous voice biomarker tracking at both individual and population levels
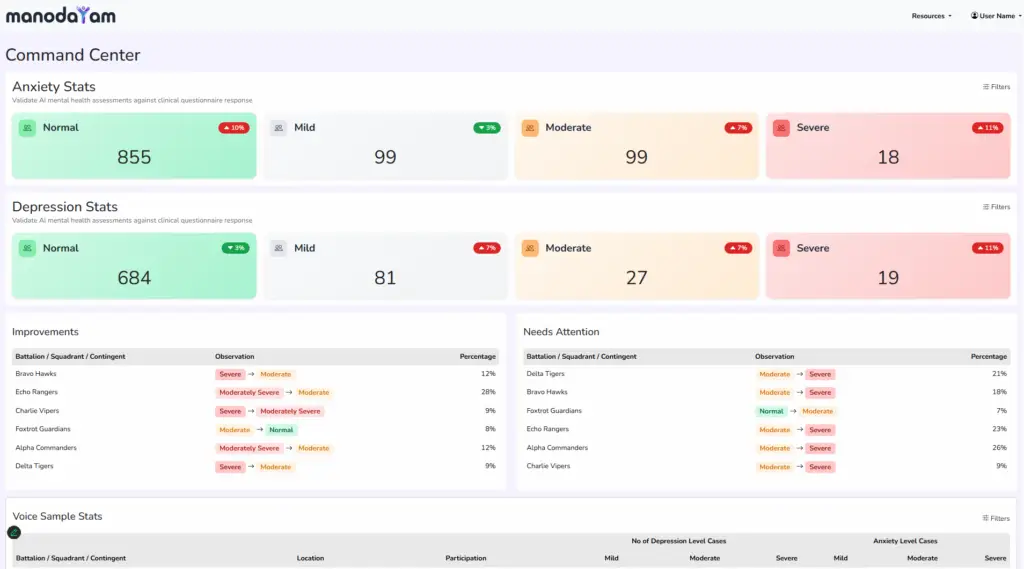
Manodayam’s advanced analytics engine processes voice biomarkers across longitudinal profiles to deliver actionable intelligence that transforms mental health from reactive crisis management to predictive population wellness

Observable Signal |
Traditional Questionnaire |
Voice Biomarker Analysis |
Clinical Relevance |
|---|---|---|---|
Vocal Energy
|
Not measured
|
Continuous tracking
|
Depression indicator
|
Pause Frequency
|
Speech rate analysis
|
Cognitive load assessment
| |
Pitch Variability
|
Not measured
|
Prosody tracking
|
Emotional state marker
|
Articulation Precision
|
Not measured
|
Formant analysis
|
Fatigue & neurodegenerative risk
|
Tremor Frequency
|
Not measured
|
Acoustic micro-tremor
|
Anxiety & PTSD marker
|
How organizations unlock intelligence from voice biomarker data
Voice biomarker analysis achieves 70-73% sensitivity and 73-75% specificity in detecting moderate-to-severe depression—comparable to or exceeding traditional questionnaires like PHQ-9. The advantage: voice analysis detects subconscious patterns (vocal energy, pause frequency, pitch variability) that people cannot consciously report. Studies show voice biomarkers predict 7-day crisis risk with 87% accuracy by detecting longitudinal deviation from individual baseline.
Voice carries 28 simultaneous biomarkers encoding emotional, cognitive, and physiological states: pitch/energy reveal emotional load; pause frequency indicates cognitive fatigue; tremor signals anxiety/PTSD; articulation precision shows fatigue/neurodegenerative risk. This happens involuntarily—subconscious markers bypass conscious filtering that questionnaires capture. No cameras (privacy), no wearables (compliance), no self-reporting bias. 10 seconds of voice = complete state-of-mind profile.
Traditional evaluation asks: “Did our program work?” (binary). Voice RCA asks: “Why did it work for some and not others?” and “What mechanism caused the observed change?” By analyzing biomarker fingerprints before/after interventions, we identify causal pathways. Example: Program X shows 12% worsening in some cohorts. Voice RCA reveals the mechanism—dosage was too high during high-stress periods. Adjustment avoids scaling failures. Research-grade RCA enables evidence-based policy iteration.
Voice data is processed through de-identification pipeline: (1) Remove identifying context (name, dates, location specifics); (2) Extract only acoustic biomarkers—pitch, energy, pause patterns—discarding actual voice content; (3) Encrypt individual-level data; (4) Aggregate for organizational/research analytics at population level; (5) 99.7% de-identification for NIMHANS/ICMR studies. Original voice is never stored long-term. Compliant with DPDP Act 2023, medical records standards, and ethics review.
Yes. AI models trained on voice cohorts differentiate: Depression (low energy, slow speech, monotonic pitch); Anxiety (high energy, rapid speech, tremor); PTSD (volatile vocal patterns, startle response); Cognitive fatigue (articulation decline, pause frequency increase); Social withdrawal (volume reduction, prosody flattening). Models achieve 70%+ accuracy for moderate-severe presentations. Mild cases and comorbidities require clinical triangulation with other assessments.
Implementation roadmap: (1) Phase 1—Baseline: Establish individual/cohort baselines over 4-6 weeks; (2) Phase 2—Integration: Embed voice collection into existing touchpoints (Tele-MANAS calls, training platforms, routine check-ins); (3) Phase 3—Real-Time Monitoring: Activate alerts for risk deviations; (4) Phase 4—Analytics: Launch dashboards for leadership and research teams. Typical deployment: 8-12 weeks for 1,000-person pilot, 6 months for institution-wide scale. ROI: ₹47 saved per ₹1 screening investment.
Manodayam enables NIMHANS/ICMR-grade research through: (1) Anonymized cohort datasets (100K+ profiles); (2) Hypothesis testing platforms for intervention trials; (3) Central data repository for meta-analyses; (4) Publication-ready visualizations; (5) Real-world evidence generation for policy papers. Partners include NIMHANS (voice biomarker validation), ICMR (multistate implementation research), universities (intervention efficacy trials). Research outputs inform National Mental Health Survey 2.0 and NMHP policy updates.
